
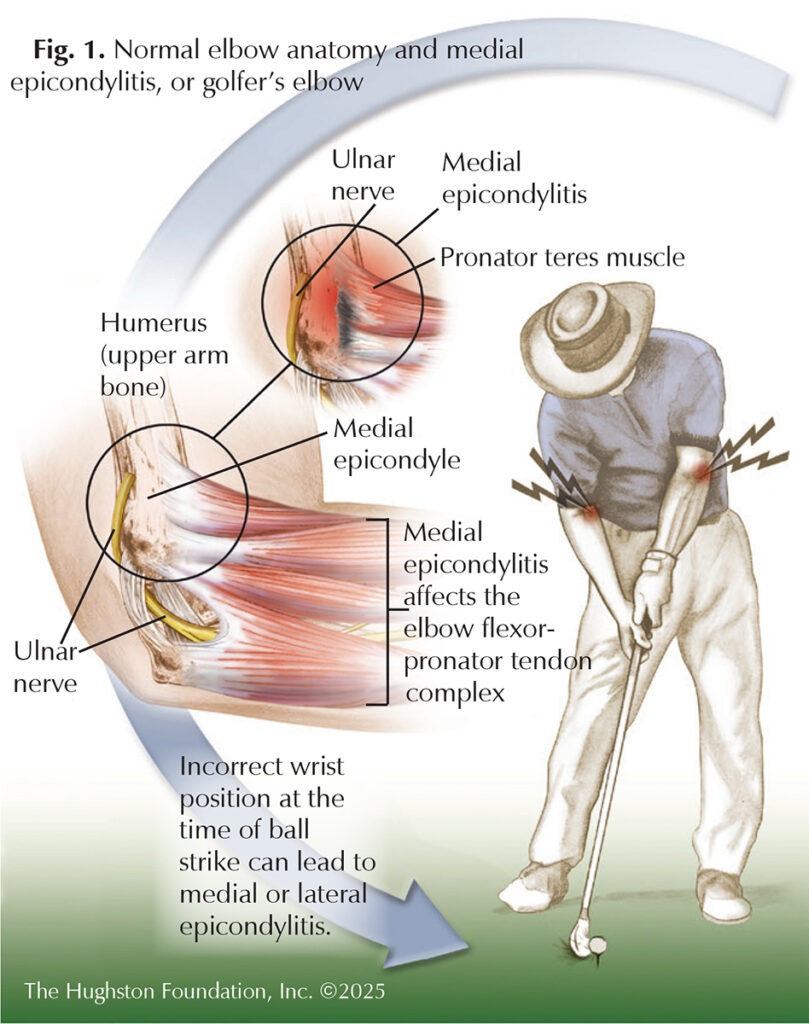
Medial epicondylitis, or golfer’s elbow, is a condition characterized by pain and tenderness on the inside of the elbow, where the tendons (tissue connecting muscle to bone) of the forearm muscles attach to the bony prominence of the medial epicondyle of the humerus (upper arm bone) (Fig. 1). It was termed “golfer’s elbow” because novice golfers who repeatedly use improper mechanics place excess stress on the pronator teres (forearm muscle) during the acceleration phase of the golf club swing. Although the condition often plagues golfers, it can be seen in baseball pitchers, tennis players, weightlifters, and individuals performing repetitive gripping or throwing motions.
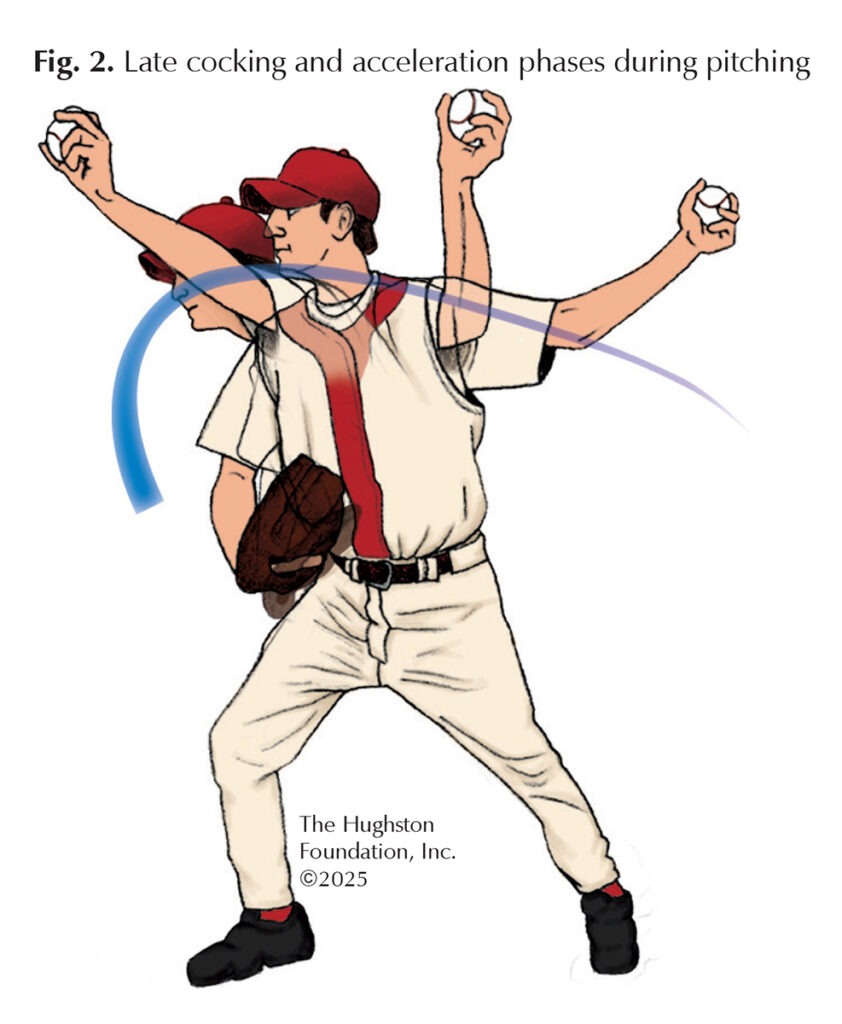 Patients who have golfer’s elbow often report pain on the inside of the elbow that worsens with activities involving wrist bending and forearm rotation, such as holding or lifting objects. For baseball pitchers, the pain can worsen during the late cocking phase—when the lead foot makes contact with the ground, and the throwing shoulder reaches maximum external rotation—or during the early acceleration phase of the throwing motion (Fig. 2). Often, the patient feels tenderness at the medial epicondyle of the humerus, and pain may radiate along the forearm. In some cases, discomfort and tendon dysfunction cause poor grip strength. Diabetics, smokers, and obese patients who endure repetitive stress on the tendon can also be affected by the condition.
Patients who have golfer’s elbow often report pain on the inside of the elbow that worsens with activities involving wrist bending and forearm rotation, such as holding or lifting objects. For baseball pitchers, the pain can worsen during the late cocking phase—when the lead foot makes contact with the ground, and the throwing shoulder reaches maximum external rotation—or during the early acceleration phase of the throwing motion (Fig. 2). Often, the patient feels tenderness at the medial epicondyle of the humerus, and pain may radiate along the forearm. In some cases, discomfort and tendon dysfunction cause poor grip strength. Diabetics, smokers, and obese patients who endure repetitive stress on the tendon can also be affected by the condition.
Diagnosis
A physical examination serves as the primary method for diagnosing the medial epicondylitis. Focused examination of the medial epicondyle and the point at which the flexor tendon attaches to the bone can help pinpoint the pain. Resisted wrist flexion and forearm pronation can reproduce symptoms, confirming the diagnosis. The physician can also test the range of motion in the affected arm to identify any limitations.
Although medial epicondylitis is primarily a clinical diagnosis, imaging such as ultrasound (uses sound waves to view inside the body) or MRI (magnetic resonance imaging scan that shows bones, muscles, tendons, and ligaments) can be used to rule out other conditions. Ultrasound can help assess tendon thickening, tears, or calcification, while MRI is beneficial for evaluating chronic cases with extensive degeneration.
Prevention
Preventative strategies for medial epicondylitis focus on minimizing the repetitive stress on the tendon. Ensuring proper mechanics to minimize strain and strengthening the forearm flexor and pronator muscles through resistance exercises can help to increase tendon durability. Incorporating stretching and warm-ups before engaging in strenuous activities, and modifying equipment to improve movement efficiency, reduces tendon stress and lowers the risk of injury.
Treatment
Initial management of medial epicondylitis includes nonoperative treatments aimed at reducing pain while promoting tendon healing. Activity modification, nonsteroidal anti-inflammatory drugs (NSAIDs), bracing, physical therapy focusing on stretching and strengthening exercises, and corticosteroid injections can encourage healing and reduce pain.1,2 If symptoms persist despite nonoperative management for at least 6 months, surgical intervention may be considered. Surgical treatment typically involves removing the damaged tendon tissue and reattaching the healthy tendon to the bone. If the ulnar nerve is affected, the surgeon can release it during the procedure.2
Untreated medial epicondylitis can also result in progressive tendon degeneration, leading to structural breakdown. The degeneration can further exacerbate pain and functional impairment.1 Additionally, due to the proximity of the ulnar nerve to the medial epicondyle, there is a risk of developing ulnar neuritis, which can manifest as numbness or tingling in the ring and little fingers.3 In severe cases, untreated medial epicondylitis may lead to partial or complete tendon rupture, which would necessitate surgical intervention for tendon debridement and repair.4 If you experience persistent elbow pain that lasts longer than 2 weeks, contact an orthopaedist for a thorough examination and treatment plan.
Author: Aneesa Jones, BS | Columbus, Georgia
References
- Amin NH, Kumar NS, Schickendantz MS. Medial epicondylitis: evaluation and management. J Am Acad Orthop Surg. 2015;23(6):348-355.
- Jobe FW, Ciccotti MG. Lateral and medial epicondylitis of the elbow. J Am Acad Orthop Surg. 1994;2(1):1-8.
- Eygendaal D, Safran MR. Postero-medial elbow problems in the adult athlete. Br J Sports Med. 2006;40(5):430-434.
- Alrabaa RG, Dantzker N, Ahmad CS. Injuries and conditions affecting the elbow flexor/pronator tendons. Clin Sports Med. 2020;39(3):549-563.
Last edited on February 26, 2026