
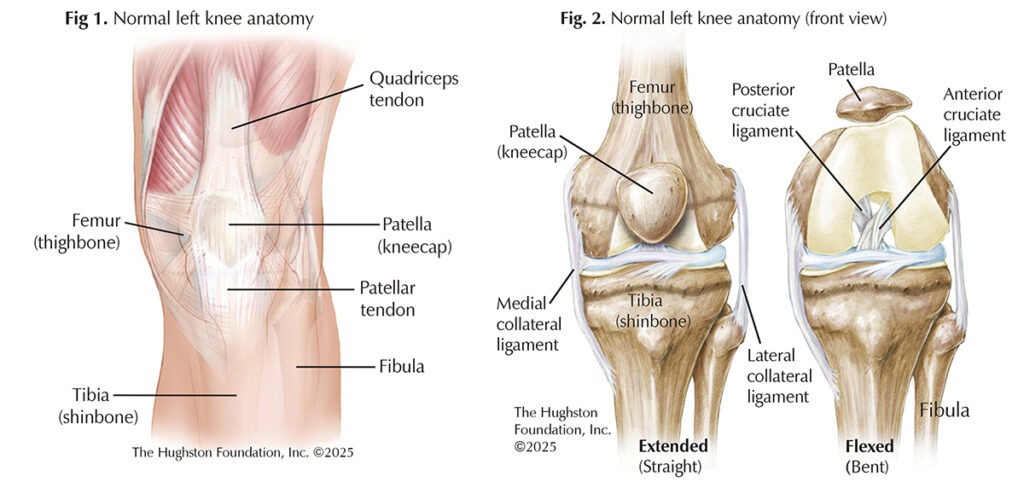
There are 4 major ligaments that stabilize the knee joint: the medial collateral, lateral collateral, anterior cruciate, and posterior cruciate. The anterior cruciate ligament (ACL) is a key stabilizer of the knee joint, and its injury is among the most common in sports medicine. When it comes to treating a torn ACL, surgical options fall into the categories of ACL repair or ACL reconstruction. While both aim to restore knee stability and function, they differ in technique, indications, and outcomes (Figs. 1 & 2).
Who injures their ACL?
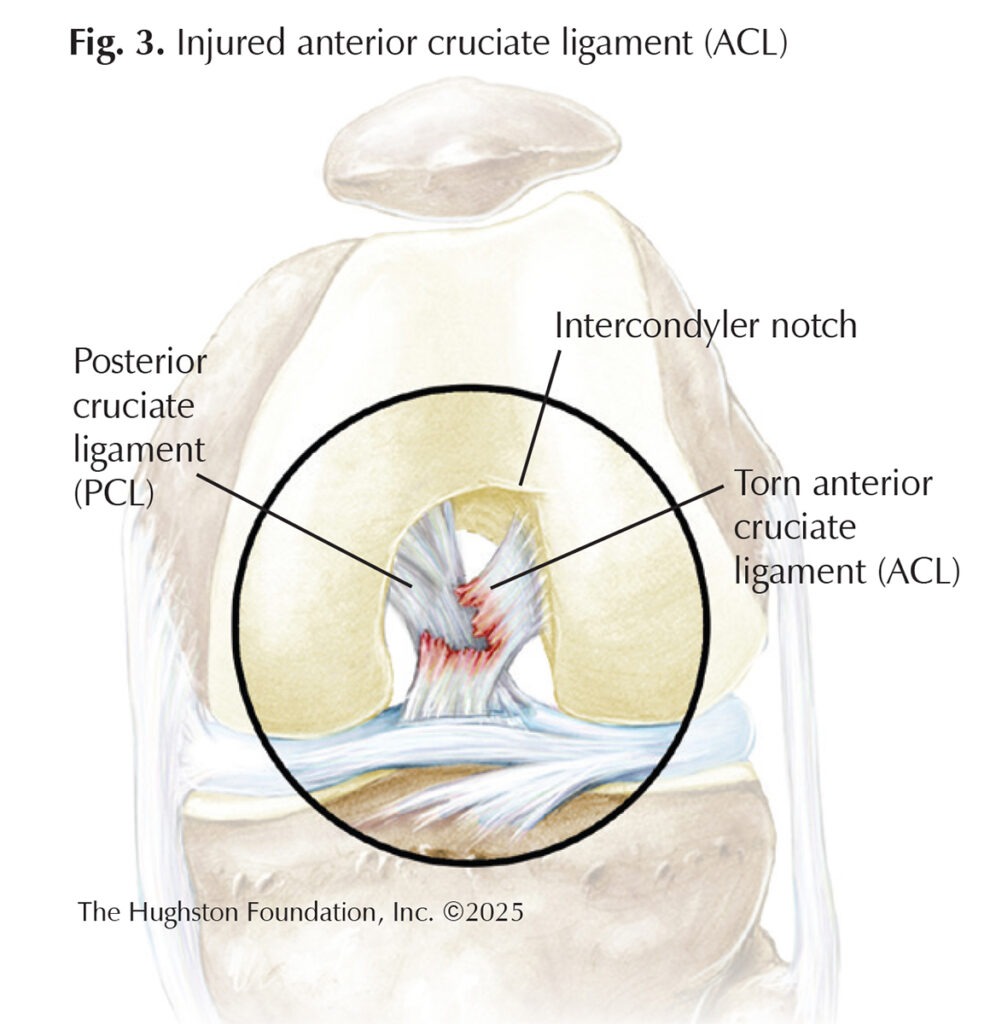
ACL injuries often occur in young, active individuals, particularly athletes involved in pivoting sports like soccer, basketball, football, and skiing (Fig. 3). Females are at higher risk than males due to anatomical and hormonal factors. The typical mechanism of injury involves noncontact movements such as sudden deceleration, change in direction, or landing from a jump.
Surgical treatment options
The choice between repair and reconstruction depends on tear type, tissue quality, and patient-specific factors. Nonoperative treatment may suffice for partial tears or low-demand individuals; however, physicians often recommend surgery for:
- Complete ACL tears in active individuals
- Combined ligament injuries
- Instability during daily activities
- Young patients at high risk for future injury
ACL repair: restoring native tissue
ACL repair involves reattaching the torn ends of the ligament to the bone. During the procedure, surgeons use an arthroscopic approach (surgery through small incisions) to re-anchor the torn ligament to the femur (thighbone) using suture anchors. Biological augmentation, using materials like platelet-rich plasma, stem cells, and growth factors, can also be used to encourage healing. This technique is most suitable for proximal (femoral-sided) avulsion-type tears with good tissue quality, typically in younger patients, and often performed early after injury. The advantages of this procedure are shorter surgical time and preservation of the native ACL structure and proprioception (body orientation). Limitations of the procedure include higher rates of retear, and it is not ideal for partial mid-ligament or chronic tears.
ACL reconstruction: the gold standard
ACL reconstruction is the most common surgical treatment, especially for midsubstance tears. It involves removing the torn ACL and replacing it with a tendon graft. A graft can be an autograft (from the patient’s body) or an allograft (donor tissue). The most common graft choices for this procedure include bone-patellar tendon-bone (BPTB), hamstring, or quadriceps tendon. The advantages of this procedure include broad applicability for all tear types, and it has been successful and stable with long-term follow-up. This procedure is more invasive, has a longer recovery time, and carries a risk of donor site complications for autografts. The procedure itself uses arthroscopic techniques to make tunnels into the femur and tibia to anchor the new graft in place.
Complications & recovery
With each procedure, there is a risk of tearing the ACL again; however, the risk is higher after repair surgery. Other complications for both procedures include stiffness, donor site pain for autograft reconstruction, graft failure with reconstruction, and a rare risk of postoperative infection in both surgical procedures. The recovery timeline for both procedures is similar, with return to work or school at 1 to 2 weeks, independent ambulation at 2 to 4 weeks, jogging at 3 to 4 weeks, and return to sport requiring 7 to 12 months.
Both ACL repair and reconstruction have valuable roles in orthopaedic practice. While reconstruction remains the standard for most ACL injuries, repair is gaining popularity for select tear types, particularly in young athletes with favorable tissue and early intervention. Shared decision-making between the patient and surgeon—based on activity level, injury pattern, and goals—is essential for optimal outcomes.
Author: Emily Jones, MD | Charleston, South Carolina
Last edited on February 26, 2026