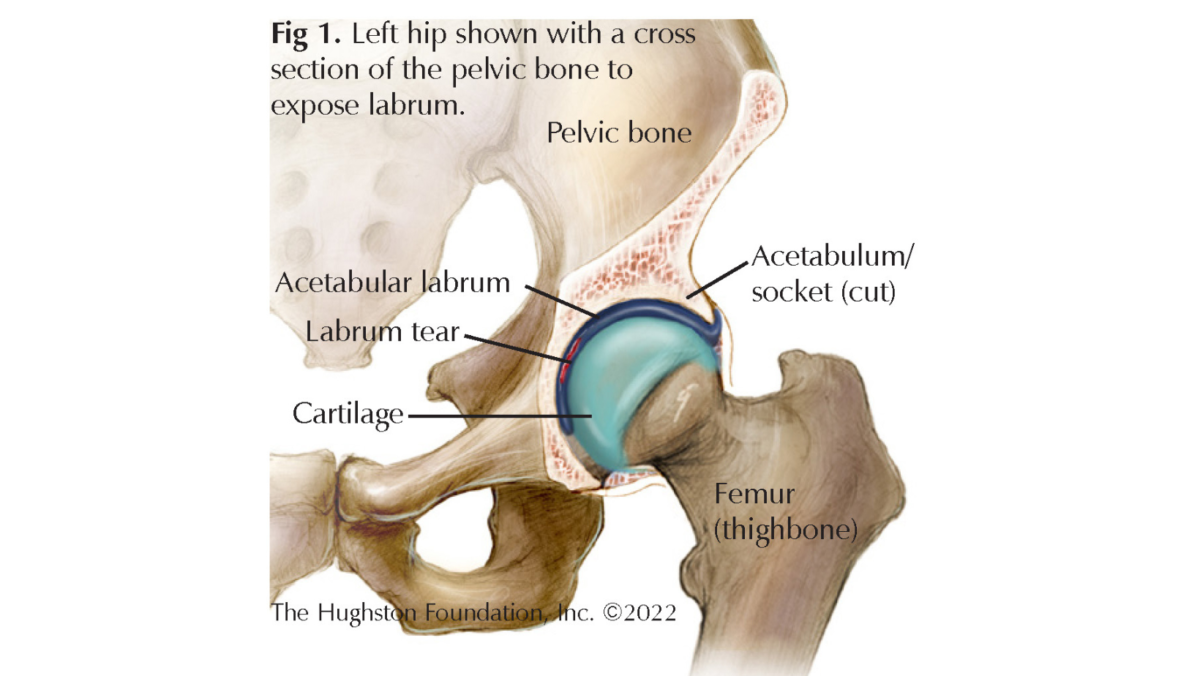
The hip joint is a ball and socket joint with a ring of cartilage that lines the socket portion of the joint called the labrum (Fig. 1). The labrum can be a pain generator in the hip if for whatever reason it becomes torn. The torn cartilage is called a hip labral tear. Diagnosing hip labral tears has increased in recent years due to the technological advancement in magnetic resonance imaging (MRI, a test that shows the bones, muscles, tendons, and ligaments) and arthroscopy (joint surgery using small incisions and a camera) that allows better visualization of the tear. Physicians often treat labral tears with conservative treatments such as rest, anti-inflammatory medication, and physical therapy, but you may need surgery if those methods do not help the pain. The pathology is common, with physicians diagnosing 22% to 55% of patients who complain of hip or groin pain with a labral tear.¹
Symptoms
Symptoms vary with some appearing suddenly, while others have a gradual onset. Patients who have a labral tear often complain of pain in the front of their hip or groin that radiates to their knee or buttock. The pain is often constant and dull and can become worse with activities such as walking, running, or prolonged sitting. In general, when patients experience pain with movement and range of motion, the pain is often sharp. You may also experience loss of range of motion, perceived instability, clicking, locking, catching, or giving way.
Risk Factors
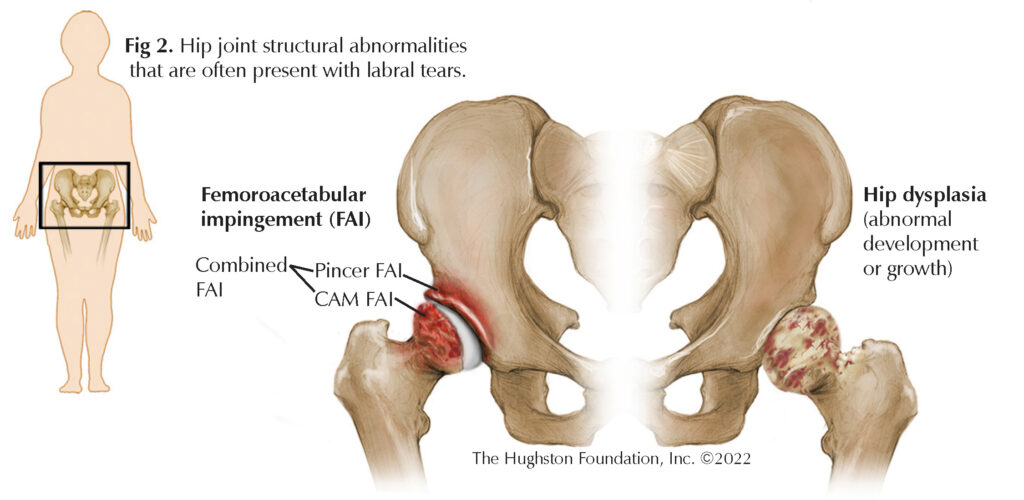
Labral tears often present with some structural dysfunction, such as femoroacetabular impingement (FAI) or dysplasia (abnormal development or growth) (Fig. 2). With FAI, the femoral head (ball portion) and neck rubs, or “impinges” on the acetabulum (socket part of the hip joint). FAI can be localized to the acetabulum, which is called Pincer FAI, or to the femur, which is called CAM FAI. It can also be due to abnormalities on both the femur and acetabulum, which is referred to as combined FAI. With dysplasia, the acetabulum does not fully cover the femur, causing increased pressure over the smaller area of the socket where the femur articulates. These conditions alter how the hip joint functions; as a result, physicians believe the labrum is more likely to tear.
Hip labral tears are more common in females rather than males and are typically in younger, active patients. Since hip labral tears are often associated with some sort of underlying structural dysfunction, the occurrence of a labral tear can coincide with the presence of articular cartilage damage or hip osteoarthritis. Therefore, an early diagnosis is key to prevent further damage to the joint.
Diagnosis
If you are experiencing continued hip pain, you should seek care from an orthopaedic specialist. When you visit the orthopaedist for hip pain, you should expect a thorough physical evaluation of your hips and lower extremities. The physician will move the hip through active and passive range of motion exercises and order x-rays or a MRI. Before the MRI begins, the radiologist may give you an injection of arthroscopic dye to help to visualize the soft tissue structures of the hip better.
Treatment
Depending on your symptoms and lifestyle, your physician can offer different treatment options. Conservative treatment can consist of rest, nonsteroidal anti-inflammatory medication, modification of activities, pain medication, physical therapy, or an intra-articular injection. Your doctor can prescribe any combination of these treatments concurrently. If conservative measures are not helpful in eradicating the pain, your doctor can recommend surgical treatment. There are multiple options for surgical treatment including labral debridement (removing the damaged part of the labrum), repair (reattaching the torn labrum to its origin), or reconstruction (where a graft is inserted in place of the torn labrum).² The surgical treatment chosen depends on the condition of the labrum. If there is an underlying cause of the labral tear, such as FAI or dysplasia, your surgeon can correct this during your labrum surgery.
Outcomes
Patients are often able to return to their prior activities after a hip labral procedure, with limitations in activities and range of motion after 4 to 6 months. Ninety-two percent of patients undergoing a labral repair procedure, report good to excellent results 3.5 years after the procedure.³ Keeping a positive attitude and adhering to your treatment and physical therapy protocols can help the recovery.
If you are experiencing hip pain that is not improving, you should seek medical care from an orthopaedic specialist. Early diagnosis is key to proper management and minimizing extended pain. It is important to discuss your symptoms and concerns with your provider in full transparency to come up with the best treatment regimen for your unique circumstances.
Author: Reily Cannon, BS, OMS-II | Henderson, Nevada
References:
- Groh MM, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskelet Med. 2009;2(2):105-117. doi:10.1007/s12178-009-9052-9 A comprehensive review of hip labral tears – PMC (nih.gov)
- Su T, Chen GX, Yang L. Diagnosis and treatment of labral tear. Chin Med J (Engl). 2019;132(2):211-219. doi:10.1097/CM9.0000000000000020 Diagnosis and treatment of labral tear – PMC (nih.gov) Hip Pain in Adults: Evaluation and Differential Diagnosis (aafp.org)
- Harris JD. Hip labral repair: options and outcomes. Curr Rev Musculoskelet Med. 2016;9(4):361-367. doi:10.1007/s12178-016-9360-9 Hip labral repair: options and outcomes – PMC (nih.gov)
Last edited on March 9, 2023