
Over the past decade, orthopaedic sports and knee injuries have been the subject of a great deal of research, which has lead to numerous advances. Following the principles of evidence-based medicine, this research has helped to improve both treatment and outcomes.
Prevention
The ultimate goal of orthopaedic research is, in fact, prevention of injury. For example, the high incidence of anterior cruciate ligament (ACL) tears in female athletes has been the subject of a great deal of investigational research. Specific studies have led to effective treatment protocols and neuromuscular training programs that improve jump landing mechanics and have produced significant injury rate reductions in female athletes. The preparticipation physical exams for ACL tears and other sports injuries in athletes has been an excellent source of data on injury rates. The exams have also proven to be an extremely valuable tool in identifying athletes who are at risk of injury and in tailoring a rehabilitation program to treat problems and reduce further damage. The Hughston Foundationsponsored Institute of Athletic Health Care and Research began performing physical exams in 1976. The database, on over 50,000 athletes, allows us to conduct research to identify the at-risk athletes and helps us to institute programs of treatment to reduce the likelihood of injury.
Diagnosis of knee injuries
Numerous advances have been made in magnetic resonance imaging (MRI) technology for the diagnosis of orthopaedic injuries. MRI technology uses a coupled magnetic field to create a scan of the bones, muscles, tendons, and ligaments. Enhancements to machine design have improved patient comfort and the speed and quality of the scans. Additionally, specific imaging protocols have led to great advances in the accurate interpretation of injury. MRI shows a higher definition of the injury, which correlates with clinical improvements and treatment outcomes whether they are operative or nonoperative.
Equipment
As in the case of conventional television, arthroscopic images have undergone evolutionary improvements in quality and detail, approaching high definition TV resolution. Better visualization of the knee during surgery greatly benefits the surgeon. In addition, numerous instruments and implants have been developed to allow many procedures to be done through the arthroscope that were all done through a large open incision 10 years ago.
Knee meniscal injuries
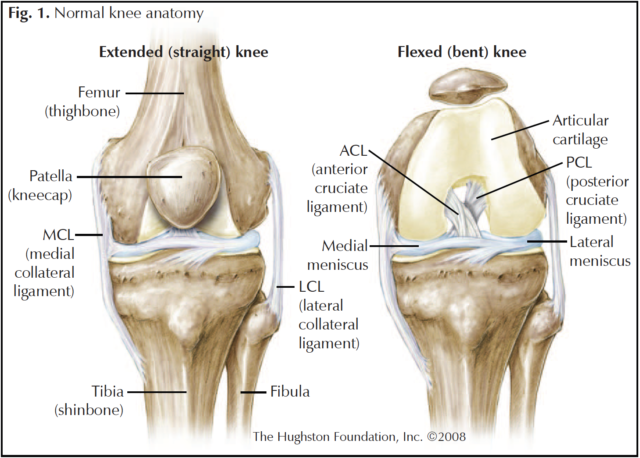
The medial and lateral menisci are very important structures located between the femur and the tibia (Fig.1). These structures help stabilize the knee, absorb impact, and provide shock absorption to the knee. When injured, the evolution and use of both clinical and MRI technologies allows us to determine the extent of injury to the meniscus. We can identify small tears that do well with nonoperative care. We can see the injury in more detail and, in many cases, that allows the surgeon to repair the torn meniscus, rather than having to remove a portion of it. Preserving the meniscal tissue leads to improved stability, decreased wear and tear, and longevity of the knee.
Knee ligament injuries
The anterior and posterior cruciate ligaments are subject to significant stress and strain during the performance of numerous athletic events. Through modern treatment techniques injuries to these ligaments can often be repaired or the ligaments can be reconstructed in a very timely fashion, allowing athletes to return to active participation in sports. Improved understanding of the anatomy, graft choices for ligament reconstruction, and rehabilitation techniques have all led to improved clinical outcomes. Although these injuries continue to be a challenge in terms of treatment, much advancement has been made.
Collateral ligament injuries have also been studied and new treatment options are now available to treat these often debilitating injuries.
Articular cartilage
The articular cartilage, (hard slippery surface that covers the ends of bones in a joint) has been the subject of a great deal of research. New techniques have been developed to restore function to injured articular cartilage. For example, treatment options to resurface injured articular cartilage run the gamut from debridement to microfracture. Debridement entails removing a flap, or unstable portion, of the damaged cartilage. And microfracture involves using a small calibrated awl to penetrate the bone beneath the cartilage to release cells from the bone marrow that can then come to the surface and grow and heal the cartilage. Certain cartilage defects also lend themselves to transplantation of small plugs of cartilage from nonweightbearing areas of the knee that can be used to fill defects in weightbearing areas. In addition, current technology allows the harvesting of cartilage cells from a patient’s knee to be grown in a culture and later reimplanted into the bone to grow a new cartilage surface. With larger defects, new allograft techniques allow replacement of both cartilage and bone with a transplant from another source other than the patient’s own tissue.
Rehabilitation
Physical therapy and rehabilitation remains a critical part of the process of treating injuries. Rehabilitation has numerous roles, to prevent further injury, treating injuries that do not need surgery, and strengthening muscles and restoring function after surgical treatment. Today, we are better able to work with Mother Nature and design earlier and more aggressive forms of rehabilitation with appropriate guidelines to shorten recovery time and to improve results.
Although many improvements have been made over the years, we remain dedicated to the research of sports injury as we look for ways to prevent injury and improve outcomes for our patients.
Author: Kurt E. Jacobson, MD | Columbus, Georgia
Last edited on May 3, 2026