
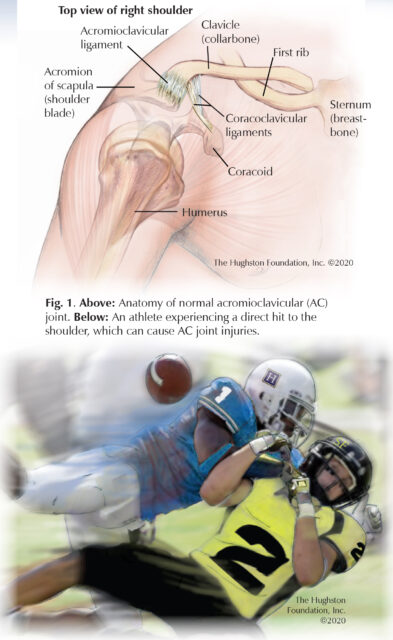
 Injury to the acromioclavicular (AC) joint is common; in fact, it makes up approximately 9% of shoulder injuries. Injury of the AC joint is often referred to as an AC sprain or an AC separation with treatment ranging from nonoperative to surgical. Orthopaedists define this injury as stretching or tearing of the ligaments (tissues that connect bones) surrounding the acromioclavicular joint and the ligaments between the coracoid and the clavicle (Fig. 1). As part of the diagnosis, doctors label the injury as a type I through a type VI, depending on the severity of the injury.
Injury to the acromioclavicular (AC) joint is common; in fact, it makes up approximately 9% of shoulder injuries. Injury of the AC joint is often referred to as an AC sprain or an AC separation with treatment ranging from nonoperative to surgical. Orthopaedists define this injury as stretching or tearing of the ligaments (tissues that connect bones) surrounding the acromioclavicular joint and the ligaments between the coracoid and the clavicle (Fig. 1). As part of the diagnosis, doctors label the injury as a type I through a type VI, depending on the severity of the injury.
The AC joint is the articulation in the shoulder between the clavicle (collarbone) and the acromion of the scapula (shoulder blade). The clavicle is the only bony connection between the arm and the axial skeleton (central bones of the chest).The AC joint is a small joint stabilized by the AC capsule, (multiple ligaments that encapsulate the joint) as well as the ligaments between the clavicle and the coracoid process (small bony projection of the scapula).
Risk factors
AC joint injuries are usually the result of a direct blow to the shoulder. The injury can occur after severe trauma, such as motor vehicle collision; but it more often happens after less severe activity such as sports participation. The injuries are prominent in contact sports, such as football, wrestling, rugby, or hockey, which may account for why male athletes are more prone to the injury than females. However, you can also experience AC joint pain from chronic irritation that results from repetitive overhead sports such as throwing a baseball, or work-related pain from doing repetitive movements on your job.
Symptoms
Patients often describe pain on top of the shoulder and can sometimes touch a specific tender area at the AC joint. You may experience increased pain while lying on your side or pain that increases with lifting or during overhead or across body movements. Upon examination, your doctor may find swelling and bruising along the shoulder, and a visible bump on the top of the shoulder. You may notice a decrease in strength and range of motion. During movement you may hear a popping sound and feel a catching sensation.
Screening and diagnosis
If you have had a shoulder injury and have either continued pain or pain with movement, you should see an orthopaedist for evaluation. Your doctor will take a thorough history, perform a physical exam, and order radiographs (x-rays) to evaluate the degree of separation. Your physician may also obtain magnetic resonance imaging (MRI scan that shows the bones, muscles, tendons, and ligaments) of the shoulder if other injuries are suspected. Injuries can range from a sprain (stretching of the ligaments) to complete tears of both the AC capsule and coracoclavicular ligaments. In the case of complete tears, the clavicle is usually significantly displaced (dislocated) from the acromion.
 Types of AC joint injuries
Types of AC joint injuries
Your orthopaedist will label your injury as a type I, II, III, IV, V, or VI, depending upon the extent of injury and number of ligaments involved. The type of injury can usually be determined with a physical examination and x-rays.
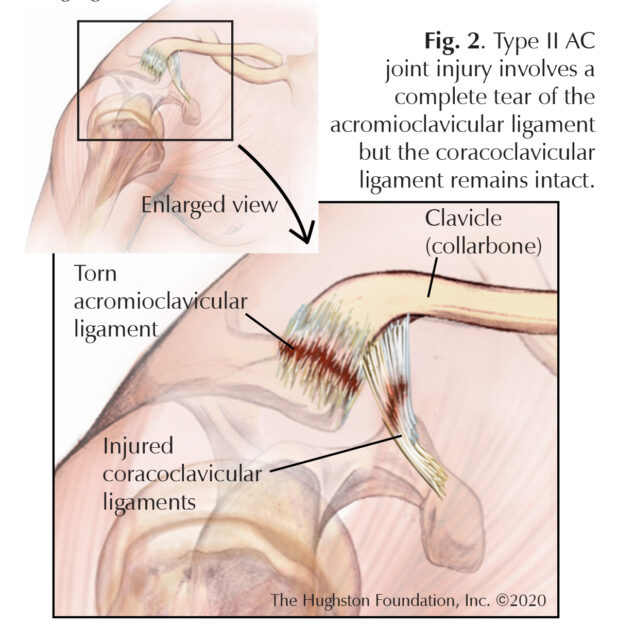
Type I injuries involve a partial tear of the acromioclavicular ligament with no injury to the coracoclavicular ligament. This causes a tender AC joint that often has mild swelling and usually heals within a few weeks. Type II injuries involve a complete tear of the acromioclavicular ligament but the coracoclavicular ligaments are stretched, but remain intact (Fig. 2). This causes a tender AC joint, often with significant swelling that heals within a few weeks. Type III injuries involve a complete tear of both the acromioclavicular and coracoclavicular ligaments. The AC joint will appear abnormal, although swelling may obscure the degree of injury. Type III injuries often take several months to heal and there is debate among surgeons on whether or not these injuries need to be fixed.
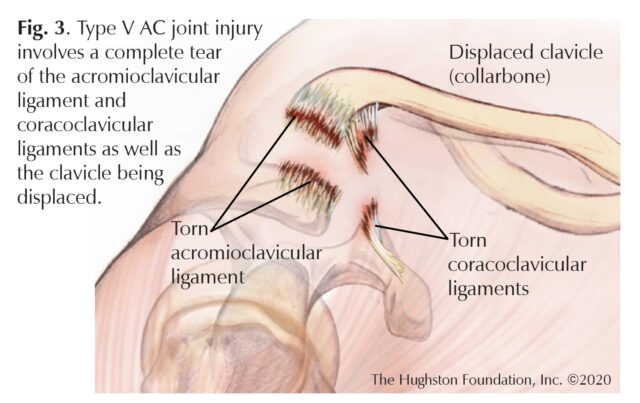
Type IV, V, VI injuries are described as the most severe cases because with these injuries both the acromioclavicular and coracoclavicular ligaments are completely torn and the clavicle is displaced (Fig. 3). During these traumatic injuries the force applied to the shoulder creates a separation between the clavicle and the acromion. Doctors distinguish these injuries by the distance and direction of the displaced clavicle. To treat these injuries, surgeons use reduction and fixation surgical treatment techniques to repair the ligaments and hold the clavicle back in its original place.
Nonsurgical treatment
If you have a type I or II injury, you may start to feel better within a few days, but it can take 6 weeks before the ligaments heal. During that time you should take the pressure off the AC joint and protect it from stretching the immature scar tissue. This would include sling immobilization for approximately 1 to 2 weeks. At follow-up, your physician will obtain repeat radiographs (x-rays) and if there are no concerning changes, such as increase in separation, you can begin gentle physical therapy that focuses on shoulder range of motion.
For more severe injuries, your doctor will work with you and a physical therapist to develop a plan for your recovery. The goal of physical therapy is to reduce pain, improve range of motion, and then to improve strength and shoulder function. After 4 to 6 weeks, most patients see improvements and can progress to advance activities as tolerated.
Surgical treatment
Most AC injuries don’t require surgery; however, more severe injuries that are associated with instability have better outcomes when operatively treated. Surgery focuses on reconstruction the coracoclavicular ligaments. Surgeons use different techniques; therefore, your surgeon will determine which treatment best fits your needs. These techniques involve suturing or using an allograft tendon (a tendon from a donor), or both, to go through or wrap around the coracoid and clavicle. Other treatments include using plates to put over the top of the clavicle and acromion. These plates can sometimes be prominent and are often removed a few months after the initial surgery. The goal of surgery is to reduce (place back into the original position) the clavicle to the acromion so that the ligaments can heal, creating scar tissue that holds the clavicle in place.
Complications
Outcomes for both nonsurgical and surgical treatments are favorable for AC joint injuries. However, complications can include chronic instability and pain if you do not seek treatment. Arthritis of the AC joint can erupt years after the injury causing residual pain between 30 to 50% of the time. Additionally, surgical fixation failure can happen, which includes loosening of the graft used to reconstruct the ligaments. Furthermore, fracture of the coracoid and clavicle can arise if tunnels are drilled within the bones during surgery.
Don’t shoulder the pain alone
AC joint injuries often result from a direct blow to the shoulder and can cause significant pain. Because the injury often results after trauma, there is no foolproof prevention plan; however, you can reduce your risk considerably by wearing protective equipment during sporting activities. Simple treatments include a short period of immobilization for mild injuries while surgery may be required for more significant injuries. Chronic symptoms can be alleviated with therapy and activity modification. For some patients, early management can prevent late complications, such as arthritis; therefore, don’t shoulder the pain alone, seek medical attention.
Author: Roman Ashmyan, DO, and Ryan Mahoney, DO | Columbus, Georgia
Last edited on July 27, 2022